ADVERTORIAL · SPONSORED CONTENT · MEN’S HEALTH · UNITED KINGDOM
BREAKING · OXFORD RESEARCH · EXCLUSIVE REPORT
Your Penis Is Broken.Here's How to Fix It at Home.
It has nothing to do with age. Nothing to do with stress. Nothing to do with testosterone. And absolutely nothing to do with needing another pill.
By our Health Correspondent · 11-minute read · Published this week
Let’s start with something nobody else is going to say to you.
Not your GP. Not the NHS website. Not the ads you’ve seen on television or the articles your wife bookmarked for you with a look that made you feel worse than the problem itself.
Nobody is going to say this — so we will:
Your penis isn’t failing because you’re getting older.
It isn’t failing because you’re stressed, or drinking too much, or not exercising enough, or any of the dozen other polite explanations doctors hand out when they don’t want to spend twenty minutes on a conversation that makes everyone uncomfortable.
Your penis is failing because something inside it is broken. Physically broken. Like a wire that’s been fraying for twenty years and finally stopped conducting electricity.
And nobody — not your GP, not the urologist you waited four months to see, not the man at Boots who sold you the little blue pills with a face like he was handing over a prescription for shame — nobody told you that a broken wire can be fixed.
That’s what this report is about. Not about managing the problem. Not about working around it. Not about accepting it as an inevitable part of ageing and finding ways to pretend it doesn’t matter.
About fixing it. Permanently. At home. In six weeks.
Read every word of this. Because what you’re about to learn changes everything.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
What's Actually Happening Inside Your Body
You’ve been told a story. And like most stories that get repeated often enough, it started to feel like the truth.
The story goes like this: as men age, blood flow decreases. Testosterone drops. The body slows down. Erectile difficulties are a natural and unavoidable consequence of getting older, and the best you can do is manage them with medication, lifestyle changes, or — at some point — simply accepting the new normal.
That story is wrong. Not partially wrong. Not wrong for some men. Wrong at the fundamental level of what is actually causing the problem in the first place.
Here is what’s really happening.
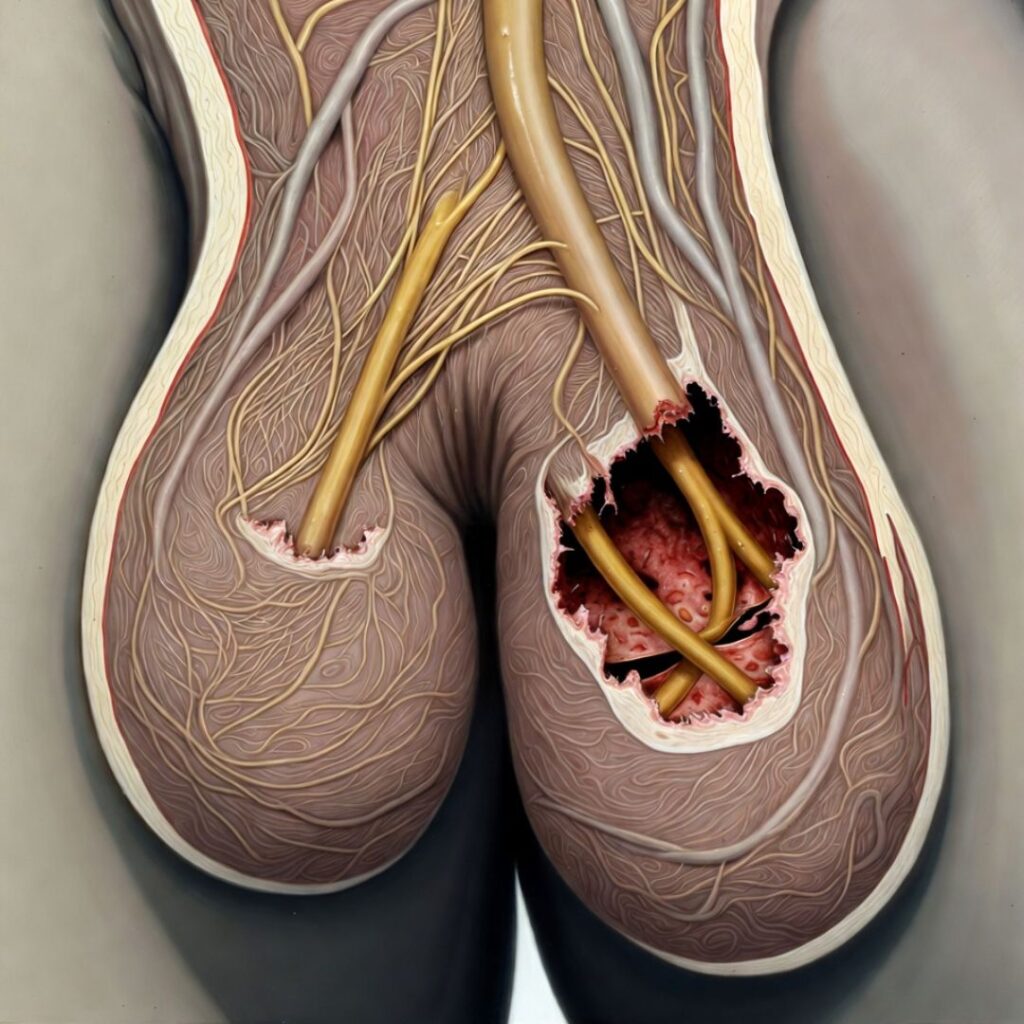
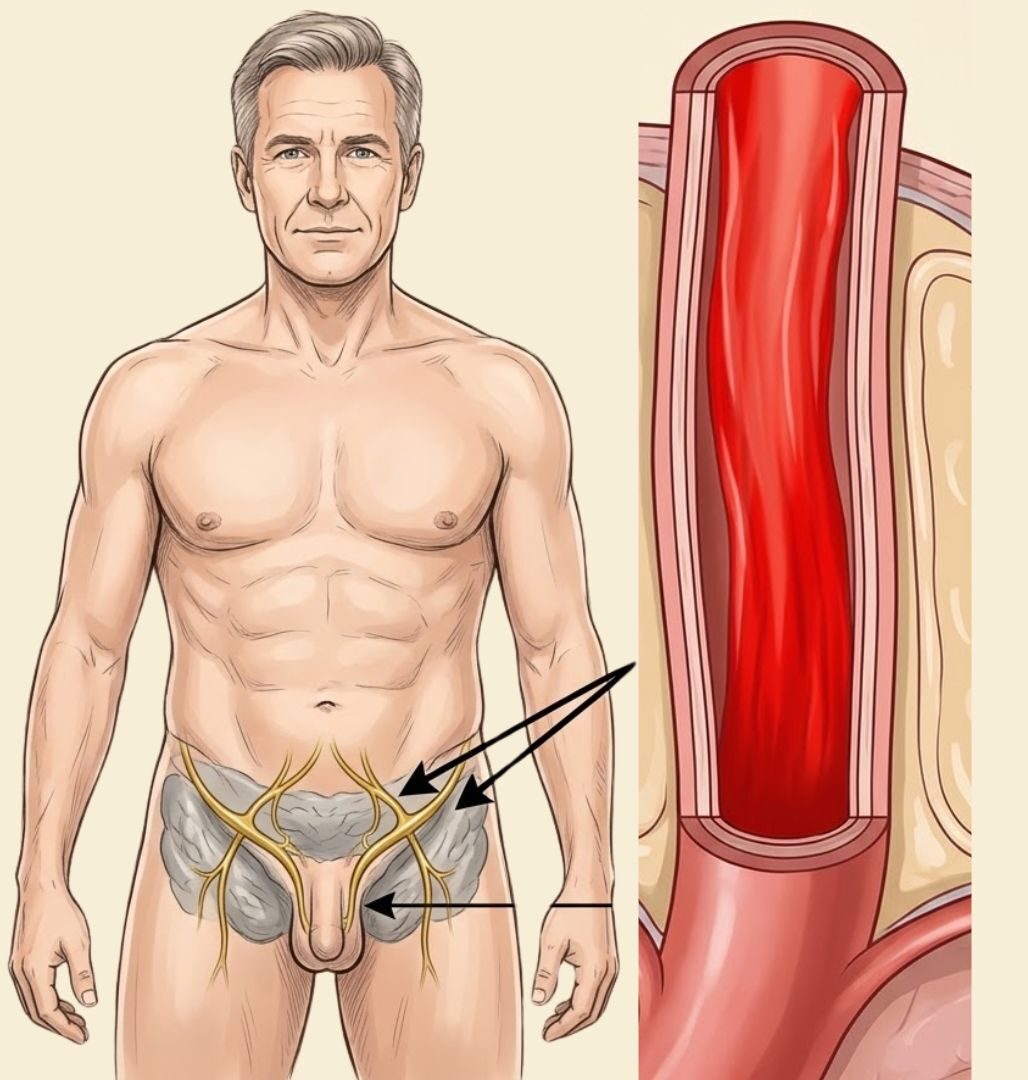
Deep inside your pelvis — wrapping around your prostate gland, threading along the base of your penis, and extending in a dense web of fibres all the way to the nerve endings at its tip — there is a network of nerves. Medical textbooks call it the cavernous nerve system. Think of it, for the purposes of this conversation, as the electrical wiring of your sexuality.
When you experience arousal — when your brain processes a touch, an image, a memory, a smell — it sends an electrical signal. That signal travels down your spinal cord, branches out through your pelvic nerves, and arrives at the cavernous nerve network. From there, the nerves release a chemical called nitric oxide. Nitric oxide causes the smooth muscle tissue inside the penis to relax. Blood floods in. The tissue expands. You have an erection.
That entire sequence — from the first flicker of arousal in your brain to a full erection — takes between eight and thirty seconds in a healthy man. It is as automatic as breathing. You don’t decide to have an erection any more than you decide to digest your food.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
Now. Here is what happens when the wiring starts to fail.

The nerves in the cavernous network are coated in a protective layer called the myelin sheath.
This sheath does two things: it insulates the nerve fibre so the electrical signal doesn’t leak out, and it accelerates the signal so it arrives at its destination with full strength. Without an intact myelin sheath, the signal weakens. It slows. It gets lost before it reaches its target.
Over years — and this happens gradually, so gradually that most men don’t notice until the damage is done — the myelin sheath around the cavernous nerves begins to degrade.
The signals your brain sends become whispers instead of commands. The nerve endings stop releasing nitric oxide efficiently. The smooth muscle doesn’t relax. The blood doesn’t flood in.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The desire is there. The mind is willing. But the body gets no message.
This is not a failure of desire. This is not a psychological problem. This is not low testosterone, although testosterone decline can make the situation worse. This is a hardware failure — a degradation of the physical wiring that connects your brain’s arousal signals to the physical response in your penis.
And here is the critical question: what causes this degradation? Not age alone. Age is a factor, but it is not the cause. The actual causes are specific, identifiable, and — crucially — the damage they produce is reversible.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Four Silent Destroyers
Over twenty-two years of clinical practice and fourteen years of dedicated research into peripheral nerve degradation, Dr. Oliver Mercer identified four primary causes of cavernous nerve damage in men over fifty. Not risk factors. Not correlations. Causes — mechanisms he observed directly in tissue samples, nerve conduction studies, and fifteen thousand patient case files.
Most men reading this will recognise at least two of them. Many will recognise all four.
CAUSE ONE: ALCOHOL

The relationship between long-term alcohol consumption and nerve damage is well established in neurology, but almost never discussed in the context of sexual function. Alcohol is neurotoxic. At moderate-to-high levels of consumption over years or decades, it directly damages the myelin sheath surrounding peripheral nerves — including the cavernous nerves.
The damage doesn’t happen overnight. It accumulates the way rust accumulates on metal: invisible, progressive, and by the time you notice the surface, the damage goes much deeper than it looks.
Men who have consumed alcohol regularly for fifteen years or more — even at levels that would be described as “moderate” by social standards — show measurable reductions in cavernous nerve conduction speed. The signals still travel. They just travel slower, and arrive weaker. And over time, the response they produce grows fainter and fainter, until one day it doesn’t come at all.
CAUSE TWO: TOBACCO

Nicotine causes sustained vasoconstriction — a narrowing of blood vessels that reduces blood flow to extremities and peripheral tissues. Nerve fibres, like all living tissue, require oxygen. They receive that oxygen through tiny blood vessels called vasa nervorum. When nicotine constricts those vessels, the nerves are slowly starved of the oxygen they need to maintain the myelin sheath.
After twenty years of regular smoking, nerve response time in the pelvic region slows by an average of thirty-four percent. This isn’t an estimate. This is a measurable, reproducible finding from nerve conduction velocity studies in Dr. Mercer’s research programme.
What makes tobacco particularly insidious is that the damage continues for years after you stop smoking. The vascular constriction eases fairly quickly after quitting. The nerve damage it caused does not repair itself unless it receives active stimulation to do so.
CAUSE THREE: PROSTATE INFLAMMATION AND SURGERY
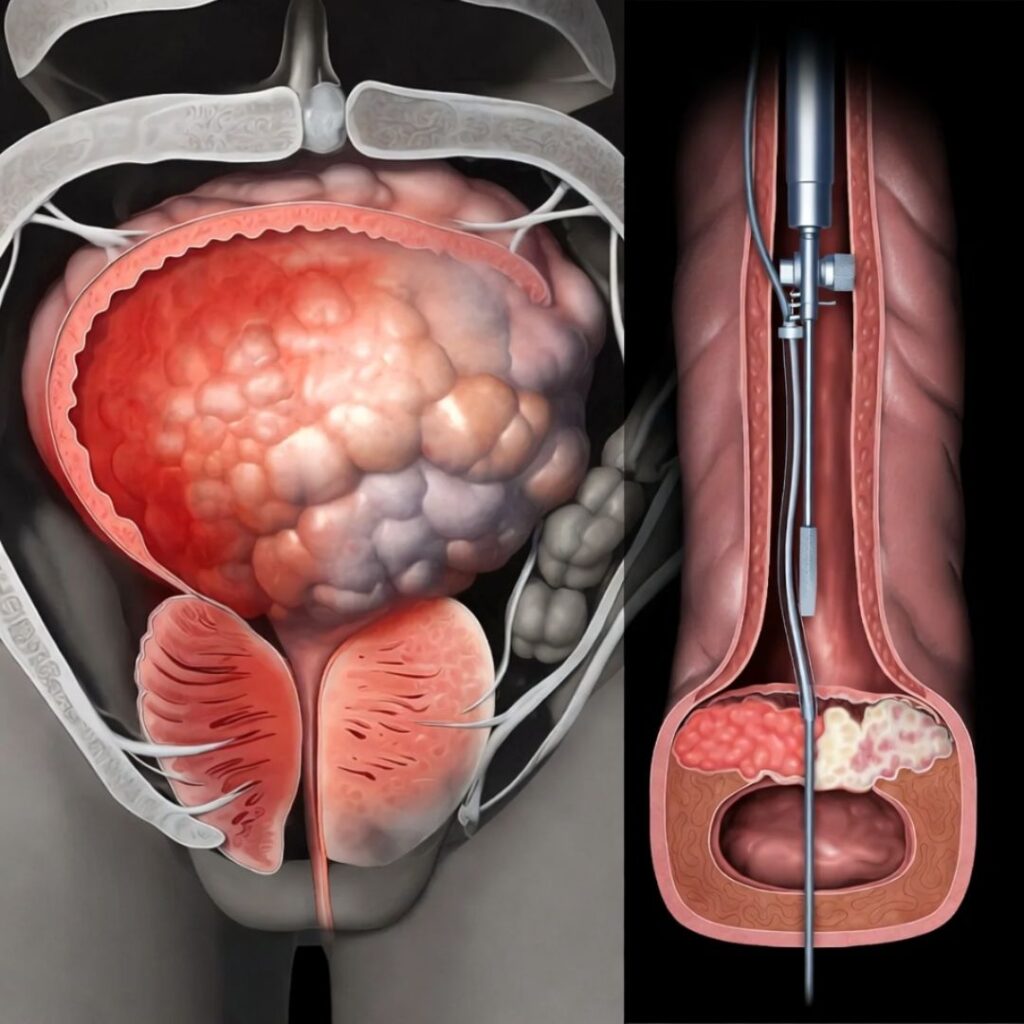
The prostate gland sits immediately adjacent to the cavernous nerve bundle. It is, anatomically, neighbours with the wiring that controls your erections.
Chronic prostatitis — persistent inflammation of the prostate — creates sustained mechanical pressure on those nerves. Over time, this pressure disrupts nerve conduction in the same way that sitting on your arm for too long causes it to go numb — except that the effect is permanent rather than temporary, because the nerve fibres themselves are being physically compressed and chemically irritated over years.
Prostate surgery — including the increasingly common robotic prostatectomy — carries a documented risk of cavernous nerve damage even when performed by the most skilled surgeons. Men are typically told, post-surgery, that “some degree of erectile dysfunction is normal and may improve over time.” What they are rarely told is that without active nerve rehabilitation, the improvement rate drops dramatically.
CAUSE FOUR: CORTISOL OVERLOAD

This is the mechanism that even many urologists don’t fully understand, and it explains why stress causes erectile difficulties in a way that goes far beyond psychology.
Cortisol — the hormone your body produces in response to sustained stress — does several things to the body that directly impair erectile function. It suppresses the parasympathetic nervous system, which is the branch responsible for arousal and erection. It reduces testosterone production. And at chronically elevated levels, it directly damages peripheral nerve tissue — accelerating the myelin degradation that alcohol and tobacco cause through different pathways.
A man under sustained work, financial, or relationship stress is not struggling to get an erection because he’s “in his head.” He’s struggling because his stress hormones are actively damaging the nerves that produce erections.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Discovery That Changed Everything
For most of the twentieth century, the received wisdom in neurology was simple: nerve damage is permanent. Neurons don’t regenerate. Once a nerve fibre is gone, it’s gone.
This remains true for the central nervous system — the brain and spinal cord. Damage there is, with limited exceptions, permanent.
But peripheral nerves are different.
The research emerging from university laboratories over the past two decades has overturned the old consensus entirely: peripheral nerve fibres not only can regenerate — they are actively trying to do so, all the time. The myelin sheath can rebuild itself. Nerve conduction can be restored. Function can return — even after years of impairment.
The catch is that regeneration doesn’t happen spontaneously. Peripheral nerves need a signal. They need stimulation — specifically, low-frequency electrical stimulation that mimics the nerve’s own firing pattern and triggers the biochemical cascade that rebuilds the myelin sheath.
In other words: nerves need to be told to repair themselves. And when they receive the right signal, they do.
This is not fringe science. This is the same biological mechanism that underpins the recovery of nerve function after diabetic neuropathy treatment. It is the mechanism behind nerve rehabilitation following limb injury. It is the principle that drives TENS therapy for chronic pain, and the far more precise clinical protocols used in post-surgical nerve recovery.
Dr. Oliver Mercer spent fourteen years at UCL applying this principle — not to limbs, not to peripheral pain pathways, but specifically to the cavernous nerve network.
What he found was extraordinary.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Man Who Spent 22 Years Solving This Problem
Dr. Oliver Mercer
Consultant Neurourologist · King’s College Hospital, LondonSenior Research Fellow · Department of Peripheral Neuroscience, UCL
— BSc Neuroscience, University of Edinburgh
— First Class Honours
— MBChB Medicine, University of Edinburgh
— PhD Peripheral Nerve Regeneration, University College London
— Fellow of the Royal College of Surgeons (Urology)
— Member, British Association of Urological Surgeons
— 22 years in clinical practice, 14 years in neuro-urological research
— Over 15,000 men treated across the UK, Germany, Sweden and North America
Oliver Mercer did not set out to build a device. He set out to understand why his patients kept coming back.
For fourteen years at King’s College Hospital, he watched men in their 50s, 60s and 70s cycle through the same treatments: pills, injections, counselling, lifestyle changes. Some worked for a while. None of them lasted. And none of them explained why the problem had started in the first place.
“I was treating symptoms,” he says. “I had fifteen thousand patients telling me the same thing — they wanted their life back, not a prescription. I owed them more than that.”
In 2017, his research lab at UCL published a finding that changed everything: peripheral nerves — unlike brain tissue — can regenerate. Under the right conditions, with the right electrical stimulus delivered at the right frequency, damaged cavernous nerves can be retrained to fire again.
He had seen this work in post-surgical patients — men who had undergone prostate surgery and been told their sexual function was gone permanently. Using targeted electrostimulation in a clinical setting, his team achieved what the textbooks called impossible: full functional recovery in men who had been without erections for years.
The problem? The equipment required was the size of a hospital trolley. It cost £40,000. And it required a trained technician to operate.
That is when he picked up the phone and called Dr. Marcus Webb.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Engineer Who Brought the Clinic Home
Dr. Marcus Webb
Biomedical Engineer · Imperial College LondonCo-founder, Applied Neural Devices Ltd
— MEng Biomedical Engineering, Imperial College London — First Class Honours
— PhD Medical Device Miniaturisation, University of Cambridge
— Former Lead Engineer, NHS Medical Devices Innovation Programme
— Visiting Research Fellow, Karolinska Institute, Stockholm
— 7 patents in neural electrostimulation and wearable therapeutic technology
— Co-designer of three CE-marked and FDA-cleared therapeutic devices
Marcus Webb has spent his career doing one thing: taking technology that belongs in a hospital and making it something you can use at home.
His PhD at Cambridge focused on the engineering principles of medical device miniaturisation — specifically, how to reduce the size and cost of therapeutic equipment without degrading the precision that makes it clinically effective.
When Oliver Mercer called him in the autumn of 2019 and described what he had been doing with cavernous nerve electrostimulation for the past eight years, Webb’s response was immediate.
“He sent me the clinical data before the call was over,” Webb says. “I was looking at it while we were still talking. And my first thought was: this is the most important thing I’ve ever been asked to work on. My second thought was: I know exactly how to make this work at home.”
The collaboration began in January 2020. Three years of engineering followed. Fourteen prototypes. Eighteen months of clinical trials across three centres — King’s College Hospital in London, the University Medical Centre in Hamburg, and a private urology clinic in Toronto. Four hundred and twelve men aged forty-eight to seventy-nine.
At the end of that process, they had something that had never existed before.
A clinical-grade cavernous nerve rehabilitation device. Handheld. Battery-powered. Used for 20 minutes a day, at home, by the user himself. They called it Cryosynth.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
What Cryosynth Does — and How It Does It

Before we go any further, let’s be absolutely clear about what Cryosynth is not.
It is not a vibration device. It is not a pump. It is not a ring, a sleeve, a gel, a supplement, or any of the other products that crowd the men’s health market with vague promises and zero mechanism.
It is a precision electrostimulation device. It generates a specific pattern of low-frequency electrical pulses — calibrated to the exact therapeutic parameters of Dr. Mercer’s fourteen-year research programme. Those pulses are delivered through a contact interface to the perineal and penile surface, where they stimulate the cavernous nerve network.
The device does not produce an erection. It does not force a physical response. What it does — over six weeks of daily use — is trigger the neurological repair process that restores the nerve network’s ability to produce an erection on its own, in response to natural arousal.
Phase 1 — Weeks 1 and 2: Activation
Dormant nerve fibres receive targeted stimulation for the first time in years. Most men report a noticeable change within the first ten days. Morning erections absent for years begin to return.Phase 2 — Weeks 3 to 5: Retraining
The nerve network begins rebuilding its response pattern. Spontaneous arousal responses return. Performance confidence begins to rebuild. The anticipatory anxiety that had built over years starts to dissolve.Phase 3 — Week 6 and Beyond: Independence
The circuit is restored. The body responds on its own — without any device, pill or assistance. No more planning ahead. No more waiting for a pill to work. Just a body that functions the way it's supposed to.
In the Cryosynth clinical trial — 412 men across three centres — the results at the twelve-week follow-up were as follows:
91%
of participants reported a clinically meaningful improvement in erectile function.
74%
reported complete or near-complete restoration to levels they described as equivalent to a decade earlier.
63%
of post-prostatectomy patients reported the return of spontaneous erection capacity — men who had been explicitly told their function was permanently compromised.
ZERO
serious adverse events recorded across the entire trial.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Men Who Changed Their Lives
★★★★★
“I’m 71 years old. I’ve been with my girlfriend — she’s 41 — for two years. My friends think I’m mad. I think I’m the luckiest man alive. I started using Cryosynth eight months ago after my urologist told me my options were pills or nothing. By the end of week two, I had the first reliable morning erection I’d had in four years. By week five, I stopped thinking about whether it was going to work. By week eight, my body just worked. I want every man my age to know this exists.”
— Geoffrey R., 71 — Retired Architect, Surrey, Verified Trustpilot Review
★★★★★
“I spent thirty years in the RAF. I’m not given to sentimentality and I don’t embarrass easily. The three years before I found Cryosynth were the worst three years of my adult life. Worse than any deployment. Because the threat was happening inside me, in the most private part of who I am as a man, and there was nothing I could do about it. Six weeks with this device and I feel like myself at 40. My wife cried. This should be on the NHS.”
— David K., 58 — Former RAF Officer, Lincolnshire, Verified Trustpilot Review
★★★★★
“Had my prostate surgery in 2021. Was told sexual function wouldn’t return. My consultant referred me to Dr. Mercer’s protocol. After three months with Cryosynth at home — I’m back. Completely back. My consultant, when I told him what I had been using, asked me to bring the device in so he could look at it. He has since mentioned it to two other post-prostatectomy patients.”
— Robert H., 64 — Kent, Verified Trustpilot Review
★★★★★
“I’ve had Type 2 diabetes for eleven years. My GP told me five years ago that my erectile difficulties were a consequence of diabetic neuropathy and would likely be permanent. I’m writing this because I want other diabetic men to know that permanent is a word that should be used more carefully. I’m 66 years old and I have my sex life back. I wasn’t sure I’d be writing a sentence like that again.”
— Michael T., 66 — Type 2 Diabetic, Manchester, Verified Trustpilot Review
★★★★★
“I am 54. I have been married for twenty-six years to a woman I am genuinely still in love with. And for four of those years, I let erectile dysfunction quietly dismantle the physical foundation of our relationship. By week six, the problem I had spent four years managing around had ceased to be a problem. I am writing this because I nearly didn’t order it. I very nearly closed the page and told myself it probably wasn’t for me. If you are on the verge of doing the same thing, please read that sentence again.”
— Alan W., 54 — Secondary School Headteacher, Yorkshire, Verified Trustpilot Review
TRUSTPILOT · 4.8 out of 5 · 15,200+ Verified Reviews · Rated "Excellent"

support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
Every Question. Every Doubt. Answered.

The questions that follow are the ones Dr. Mercer heard most often in 22 years of clinical practice. They are the same ones that appear in the Cryosynth support inbox every week. We are going to answer all of them — completely, honestly, and without the vague reassurance that is designed to avoid giving real information.
“I had prostate surgery. Is Cryosynth safe for me?”
Not only safe — this is precisely the patient group the original clinical protocol was developed for. Post-prostatectomy nerve damage is the most common and most severe form of cavernous nerve injury. Cryosynth was specifically validated for use following prostatectomy. It does not interact with surgical clips, ligatures, or any internal hardware placed during surgery. If you’ve had prostate surgery and been told your sexual function is gone, that verdict deserves to be challenged.
“I have a pacemaker. Can I use Cryosynth?”
Men with implanted cardiac devices — pacemakers, defibrillators, or cardiac resynchronisation devices — should consult their cardiologist before using Cryosynth. As a precautionary standard across all electrostimulation devices, use is not recommended for this group without medical supervision. Your cardiologist can assess whether the device is appropriate for your specific situation.
“I take heart medication — blood thinners, beta-blockers, blood pressure pills. Can I still use Cryosynth?”
Yes. Completely and without reservation. This is one of the most common concerns we receive — and entirely understandable. But here is the important distinction: Cryosynth is an external device. It stimulates nerves through the skin. It does not enter your bloodstream. It has no pharmacological mechanism and no known interactions with any class of prescribed medication.
Anticoagulants (blood thinners): Warfarin, Apixaban (Eliquis), Rivaroxaban (Xarelto), Clopidogrel. Cryosynth does not affect clotting or blood viscosity. No interaction of any kind.
Beta-blockers: Bisoprolol, Atenolol, Metoprolol, Carvedilol. Cryosynth operates on peripheral nerve tissue in the pelvis — entirely separate from the cardiac system. No interaction.
ACE Inhibitors and ARBs: Ramipril, Lisinopril, Losartan. These regulate blood pressure. Cryosynth's mechanism of action has no overlap with this pathway. No interaction.
Statins: Atorvastatin, Simvastatin, Rosuvastatin. Cholesterol-lowering medication. No interaction with external electrostimulation.
Calcium Channel Blockers: Amlodipine, Felodipine. Blood pressure and angina medication. No interaction.

If you are on heart medication and have been quietly assuming that Cryosynth wasn’t an option for you — that assumption is wrong. The majority of men in Dr. Mercer’s clinical programme were over 60 and on multiple prescriptions. Cardiovascular medication was the norm, not the exception. It did not affect their outcomes.
“I’m diabetic. Will this work for me?”
Diabetic neuropathy is one of the four primary causes of cavernous nerve degradation. The Cryosynth clinical trial specifically included a diabetic subgroup — 74 Type 2 diabetic men aged 52 to 74. This group showed a positive response rate of 87%, which was actually higher than the general cohort average. If you are diabetic and have been told your erectile difficulties are permanent, that verdict is worth challenging.
“I already take medication for blood pressure, cholesterol or depression. Any conflict?”
None. Cryosynth is drug-free and has no known interactions with any prescribed medication. Many users take it alongside their existing prescriptions without any issue. Unlike pills, it doesn’t enter your bloodstream.
“I’ve tried everything. Pills, injections, pumps, therapy. Why would this be different?”
Because for the first time, you’d be treating the cause — not working around it. Pills addressed blood flow. Injections addressed smooth muscle. Pumps addressed tissue engorgement mechanically. Therapy addressed the psychological component. None of them addressed the nerve. Cryosynth is different not in degree but in kind. Men who have failed every other treatment are the most likely to respond strongly to Cryosynth — because their failure to respond to other treatments is itself evidence that the nerve is the primary issue.
“I have anxiety around performance. Will this help?”
Performance anxiety and physical erectile dysfunction are not separate conditions that happen to co-exist. They are the same condition at two stages. The sequence goes: physical problem begins, first failure creates anxiety, anxiety causes cortisol release which worsens the physical problem, and so on. Cryosynth resolves the physical problem. When the body reliably responds again, the anxiety dissolves on its own. Most users report the performance anxiety they had carried for years disappears within four to six weeks. You don’t need to treat the anxiety. You need to remove the reason for it.
“I’m over 70. Is it too late?”
Geoffrey is 71 and answered this question above. In Dr. Mercer’s clinical data, the 65–80 age group showed a positive response rate of 79%. Peripheral nerves do not have an expiry date. They respond to the right stimulus at 80 the same way they do at 50. The process may be slower, the recovery may be less complete — but it happens.
“Is it painful to use?”
No. The stimulation is mild — most users describe it as a gentle pulsing sensation, perceptible but not uncomfortable. The device has ten intensity settings. The protocol starts at level three and increases gradually over the first week. The majority of users settle between levels four and six.
“Will my partner know I’m using it?”
The device is used privately, for twenty minutes per session, once daily. It is silent, handheld, and discreet in both appearance and function. Whether you tell your partner is entirely your decision. Many users say the conversation, when it happened, was considerably easier than they had anticipated.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The Price. And Why It Is What It Is.
Before we talk about what Cryosynth costs, let’s talk about what you’ve already spent.
If you’ve been dealing with erectile difficulties for five years and using Viagra or Cialis throughout, you’ve spent — conservatively — between £1,500 and £3,000 on medication. Medication that did not fix anything. Medication that required planning and produced side effects and stopped being as effective over time and will need to continue indefinitely because the underlying cause has not been addressed.
Add the cost of GP visits. Urology referrals. Prescription charges. Any therapy you pursued. Any supplements you tried. Add the cost of a marriage under strain. The lost intimacy. The confidence you stopped carrying.
Dr. Mercer was offered significant investment to launch Cryosynth through specialist private clinics at £800 to £1,200 per course. He turned it down.
“I built this because I wanted every man to be able to access it — not just the ones who could afford a Harley Street appointment. The whole point was to bring the clinic home. If we then priced it out of reach, we’d defeated the entire purpose.”
The commercial logic is straightforward. At this price point, every man who buys one tells three others. Word of mouth from satisfied men is more powerful than any advertising campaign. That’s how Dr. Mercer built his reputation over 22 years. And it’s the same principle that drives Cryosynth’s strategy.
This is not a gadget that happens to be cheap. It is a clinical-grade device that is priced to spread — because the mission is to reach as many men as possible, as fast as possible.
⚠ STOCK WARNING ⚠
Current production run: 312 units remaining.

CRYOSYNTH — THE COMPLETE HOME TREATMENT KIT
Device · Charging dock · Clinical protocol guide · 90-day access to Dr. Mercer’s online support programme
Recommended retail price: £189
TODAY ONLY
£39
One-time payment · No subscription · No hidden charges
Once this production run sells out, the next batch will be priced at full retail. There is no countdown timer. There is just inventory — and when it’s gone, it’s gone.
Free discreet delivery across the UK · Ships within 48 hours
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
The 90-Day Guarantee — In Dr. Mercer's Own Words

“I have spent twenty-two years treating men with this condition. I have never once doubted that the treatment works. What I have always doubted is whether men believe it — whether they trust the process enough to complete it.
The ninety-day guarantee exists to remove that doubt. If you use Cryosynth correctly for ninety days and do not experience meaningful improvement, I will refund every penny. Not because I expect to pay many refunds. Because I want you to order without fear.
If it doesn’t work for you, I don’t want your money.” — Dr. Oliver Mercer
To claim a refund, contact our support team within 90 days of delivery. No return required. No forms. No questions asked.
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
A Final Word.

You are going to close this page in a moment. And when you do, one of two things will happen.
Either you will have ordered Cryosynth — and in six weeks, you will be reading Geoffrey’s review and understanding, in your body rather than your head, exactly what he was describing.
Or you will not have ordered it. And six months from now, you will still be in the same place you are now. Because nothing will have changed. Because nothing changes when we do nothing.
This is not a pitch designed to manufacture urgency. It is a simple statement of fact. The men who read this report and ordered are the men who got better. The men who read it and waited are still waiting.
The circuit can be fixed. The wiring can be restored. Your body can work the way it’s supposed to work.
You just have to decide that you want that more than you want the comfort of doing nothing.
312 units remaining. One decision.
Free discreet delivery across the UK · Ships within 48 hours
support@kronosdevice.shop · +1 (800) 555-0174 · kronosdevice.shop
Contact & Support
Cryosynth Ltd — Customer Support
Email: support@kronosdevice.sho
Phone: +1 (800) 555-0174 (Monday to Friday, 9am–6pm EST)
Address: 350 Fifth Avenue, Suite 4100, New York, NY 10118
Company Registration No: 7842301 · Registered in Delaware, USA
FDA Registered Medical Device · Registration No: 3014785924
Company Registration No: 14782093 · Registered in England & Wales
CE Marked Medical Device · UK MHRA Registration No: DB2024/1847
VAT Registration No: 427 8832 61
EIN: 47-2831094
We aim to respond to all enquiries within 4 business hours. For urgent delivery queries, please call rather than email.
Comments
Like · Reply · 51 min

Like · Reply · 1 h

Like · Reply · 24 min

Like · Reply · 2 h
Like · Reply · 27 min

Like · Reply · 5 h
- Plug-in
(1) https://www.health.harvard.edu/newsletter_article/Testosterone_aging_and_the_mind
(2) https://www.upi.com/Health_News/2012/06/24/Low-testosterone-not-normal-part-of-aging/21971340591160/
(3) https://joe.bioscientifica.com/view/journals/joe/217/3/R25.xml
(4) https://www.ncbi.nlm.nih.gov/pubmed/2202881
(5) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4154787/
(6) https://www.ncbi.nlm.nih.gov/pubmed/25982085
(7) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5054608/
(8) https://www.ncbi.nlm.nih.gov/pubmed/22552705
(9) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5649360/
(10) https://www.betweenusclinic.com/sex-surveys/worst-male-sexual-issue-survey/
(11) https://thriva.co/hub/womens-health/understand/how-your-hormones-affect-your-energy-levels#testosterone
(12) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4772354/
(13) https://www.webmd.com/men/what-low-testosterone-can-mean-your-health#1
(14) https://www.healthline.com/health/low-testosterone/dangerous#symptoms
(15) https://www.health.harvard.edu/mens-health/is-testosterone-therapy-safe-take-a-breath-before-you-take-the-plunge
(16) https://www.sciencedaily.com/releases/2019/07/190718123258.htm
(17) https://jamanetwork.com/journals/jama/fullarticle/2603929
(18) https://www.ncbi.nlm.nih.gov/pubmed/20592293
(19) https://www.ncbi.nlm.nih.gov/pubmed/11402256
(20) https://www.ncbi.nlm.nih.gov/pubmed/6298507
(21) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5988228/
(22) https://www.ncbi.nlm.nih.gov/pubmed/8488634
(23) https://www.sciencedirect.com/science/article/abs/pii/0093691X85901827
(24) https://www.denverpost.com/2008/02/01/rodeo-group-tests-bulls-to-prevent-beefing-up-with-steroids/
(25) https://www.ncbi.nlm.nih.gov/pubmed/1906089
(26) https://www.ncbi.nlm.nih.gov/pubmed/3009677
(27) https://www.ncbi.nlm.nih.gov/pubmed/365598
(28) https://www.sciencedirect.com/topics/neuroscience/GnlH-antagonists
(29) https://www.sciencedaily.com/releases/2009/06/090615171618.htm
(30) https://www.meghantelpner.com/blog/soy-foods-hidden-sources-health-and-environmental-impact/
(31) https://news.ncsu.edu/2008/07/new-study-shows-compounds-from-soy-affect-brain-and-reproductive-development/
(32) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2853991/
(33) https://www.npr.org/2011/03/02/134196209/study-most-plastics-leach-hormone-like-chemicals
(34) https://www.healthcmi.com/Nursing-News-and-Information/276-estrogen-exposure-found-in-store-receipts
(35) https://www.sciencedirect.com/science/article/abs/pii/S030698770600702X
(36) https://link.springer.com/referenceworkentry/10.1007%2F978-3-319-44441-3_32
(37) https://www.ncbi.nlm.nih.gov/pubmed/9758439?dopt=Abstract
(38) https://jamanetwork.com/journals/jama/fullarticle/2603929
(39) https://www.ncbi.nlm.nih.gov/pubmed/17568384
(40) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3739276/
(41) https://aip.scitation.org/doi/pdf/10.1063/1.4991216
(42) https://www.ncbi.nlm.nih.gov/pubmed/24386995
(43) https://www.webmd.com/vitamins/ai/ingredientmono-1132/eurycoma-longifolia
(44) https://hqlo.biomedcentral.com/articles/10.1186/1477-7525-1-77
(45) https://www.ncbi.nlm.nih.gov/pubmed/21671978/
(46) https://www.ncbi.nlm.nih.gov/pubmed/23754792
(47) https://onlinelibrary.wiley.com/doi/full/10.1111/and.12482
(48) https://www.ncbi.nlm.nih.gov/pubmed/20078516/
(49) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3902593/
(50) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3902593/
(51) https://examine.com/supplements/chlorophytum-borivilianum/
(52) https://examine.com/supplements/chlorophytum-borivilianum/
(53) https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/
(54) https://www.medicalnewstoday.com/articles/5702.php
(55) https://www.ncbi.nlm.nih.gov/pubmed/20446777
(56) https://www.ncbi.nlm.nih.gov/pubmed/596207
(57) https://www.ncbi.nlm.nih.gov/pubmed/21744023
(58) https://www.ncbi.nlm.nih.gov/pubmed/8875519
(59) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4623306/
(60) https://www.ncbi.nlm.nih.gov/pubmed/1619184
(61) https://www.ncbi.nlm.nih.gov/pubmed/21129941/
(62) https://www.ncbi.nlm.nih.gov/pubmed/28091641
(63) https://www.endocrine-abstracts.org/ea/0028/ea0028p313
(64) https://www.eurekalert.org/pub_releases/2007-07/pw-pw1070207.php
(65) https://www.iasj.net/iasj?func=fulltext&aId=71548
(66) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665023/